Why this topic matters in Illinois
• Heart disease remains the leading cause of death in Illinois (26,280 deaths in 2021). Stroke is fifth; together they account for ~27% of statewide deaths. [1]
• The 2025 age‑adjusted heart‑disease mortality rate in Illinois is ~161 per 100,000, underscoring the value of prevention. [2]
Where Homocysteine and Heart Health fit in Illinois (2025)
–Meet homocysteine (and your “one‑carbon” engine)
• Homocysteine forms naturally as your body uses methionine.
• Two main routes handle it:
– Remethylation: homocysteine → methionine (needs folate as 5‑MTHF + vitamin B12 as a cofactor).
– Transsulfuration: homocysteine → cystathionine → cysteine (needs vitamin B6/PLP).
• Methionine makes SAMe (S‑adenosylmethionine), the universal methyl donor for DNA and neurotransmitter chemistry. [3][4][5][6]
-What the number means (quick visual)
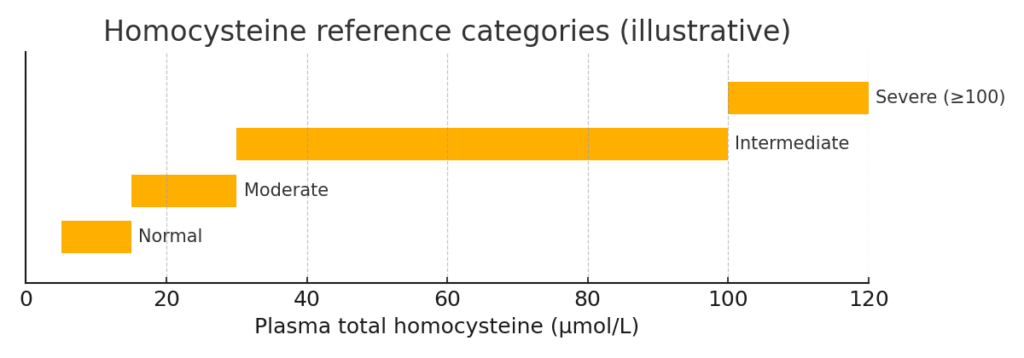
• Typical lab categories (µmol/L): Normal 5–15; Moderate 15–30; Intermediate 30–100; Severe ≥100. [7]
• Chart: Homocysteine reference categories
What the best evidence says (and doesn’t)
-Observational links vs. randomized trials
• Observational data: higher homocysteine tracks with higher cardiovascular risk. [8]
• Randomized trials: lowering homocysteine with folic acid/B‑vitamins reliably drops the lab number but doesn’t consistently prevent heart attack or major events in fortified countries; some stroke benefit appears in low‑folate settings. [9][10][11]
• Bottom line for U.S./Illinois: the number is a marker, not a magic lever for outcomes. [12]
-When testing may be reasonable
• Suspected vitamin B12 or folate deficiency (homocysteine rises early).
• Rare inborn errors (e.g., classical homocystinuria) when clinically suspected.
• Clinical decisions would change based on the result.
• Not recommended for routine cardiovascular risk screening in otherwise stable adults (per ACC/AHA guidance). [3][4][7][12]
About MTHFR genotype: what matters and what doesn’t
-The variants, in one glance
• Common variants: C677T and A1298C.
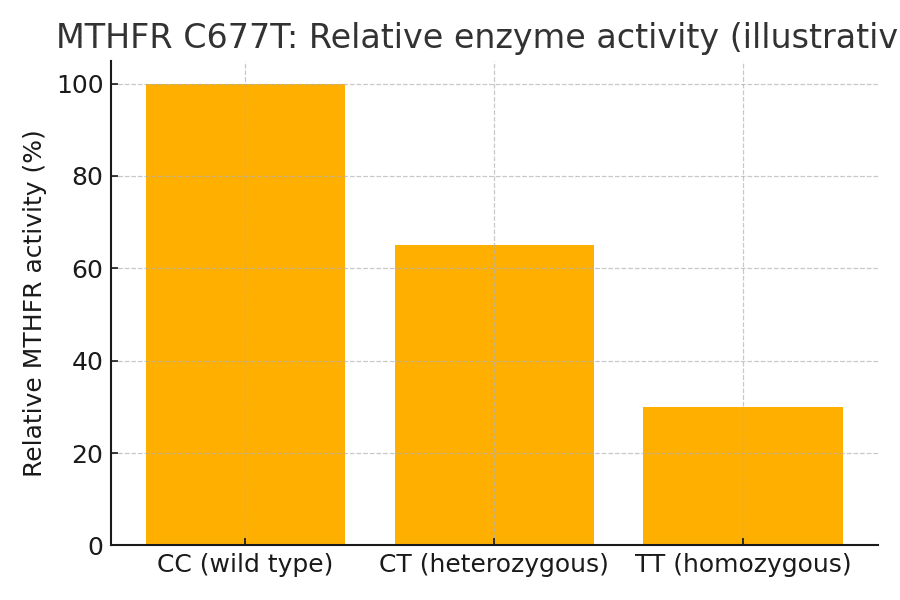
• C677T: average enzyme activity ≈100% (CC), ≈65% (CT), ≈30% (TT).
• A1298C: reduced activity, typically less than C677T’s effect. [13][14]
• Chart: Estimated relative MTHFR activity by genotype
-Why the U.S./Illinois context is different
• Since 1998, many U.S. grain products have been fortified with folic acid, improving folate status and blunting the homocysteine effect of MTHFR variants. [15]
• Fortification helped reduce neural tube defects; it also helps explain why B‑vitamin trials in fortified populations seldom show big cardiac gains. [11][15]
-Should you order MTHFR testing?
• Major genetics and public‑health groups advise against MTHFR genotyping for cardiovascular risk or thrombophilia evaluations; it rarely changes care. [16][17][18]
• Focus on modifiable risks and when indicated, the actual homocysteine value.
Food first: practical ways to support a healthy balance
-Folate (vitamin B9)
• Role: supplies 5‑MTHF for remethylation. [4]
• Illinois‑friendly foods: spinach, kale, broccoli, beans/lentils, oranges; enriched breads, pasta, rice, and many cereals (fortified with folic acid). [4]
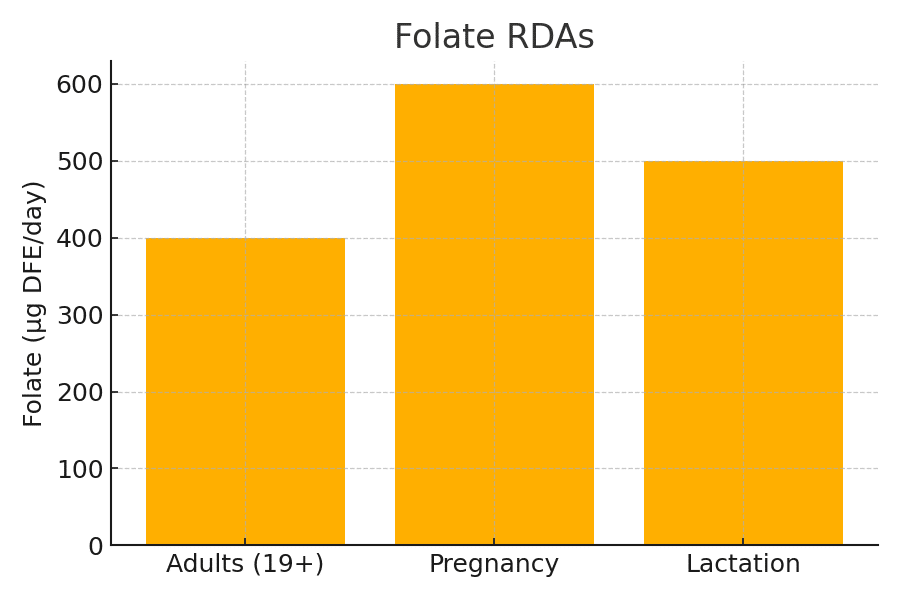
• RDA targets (µg DFE/day): Adults 400; Pregnancy 600; Lactation 500. [4]
• Chart: Folate RDAs
-Vitamin B12 (cobalamin)
• Role: cofactor for methionine synthase; critical for SAMe. [3][6]
• Foods: clams, salmon/tuna, lean beef, dairy, eggs; fortified cereals/plant milks for plant‑forward eaters. [3]
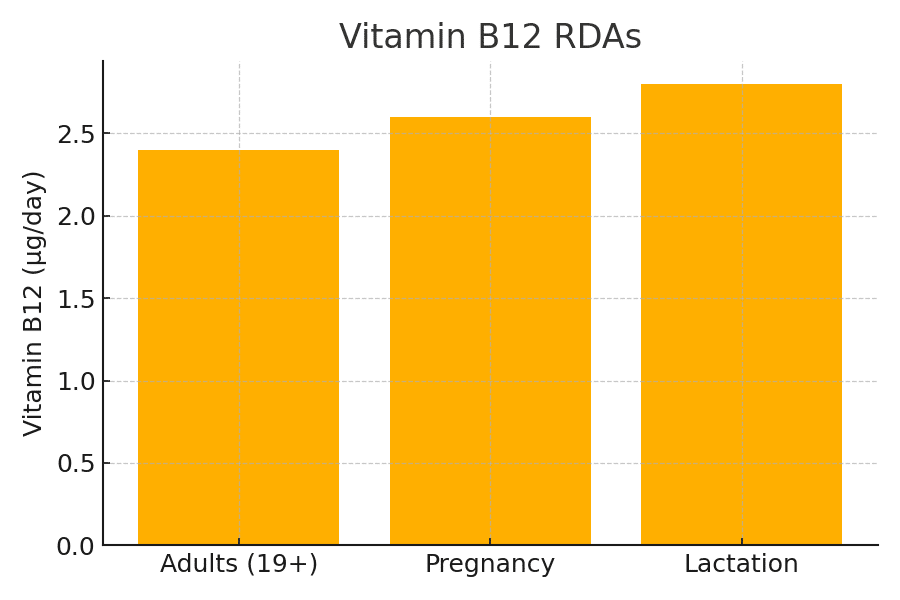
• RDA (µg/day): Adults 2.4; Pregnancy 2.6; Lactation 2.8. [3]
• Chart: Vitamin B12 RDAs
-Vitamin B6 (pyridoxine)
• Role: coenzyme (PLP) for transsulfuration. [5]
• Foods: chickpeas, potatoes, poultry, tuna/salmon, bananas, fortified cereals. [5]
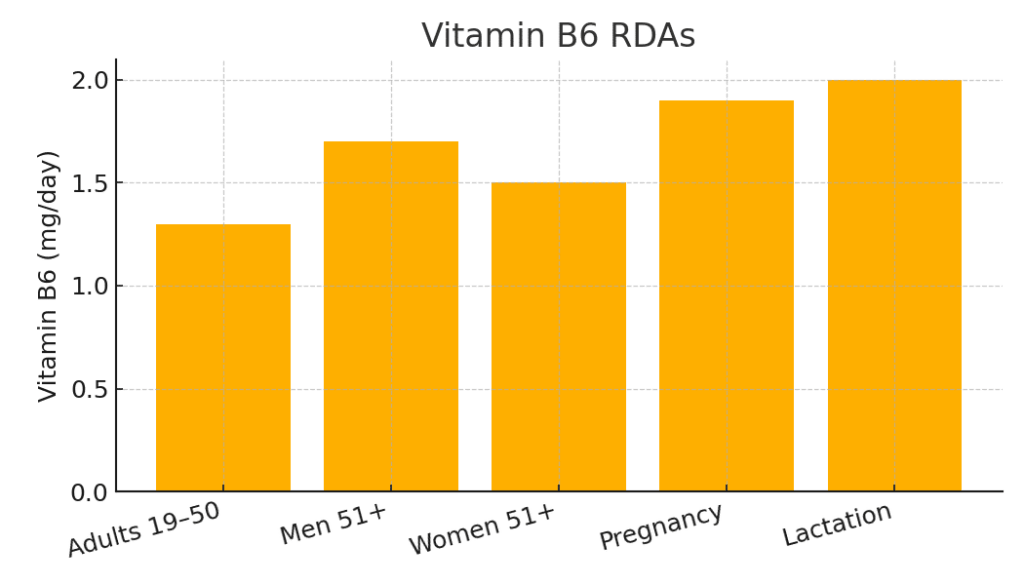
• RDAs (mg/day): Adults 19–50: 1.3; Men 51+: 1.7; Women 51+: 1.5; Pregnancy 1.9; Lactation 2.0. [5]
• Chart: Vitamin B6 RDAs
-Smart shopping in Illinois
• Enriched grains statewide contain folic acid by mandate; corn masa flour fortification is voluntary—check labels if masa is a staple. [15][19]
• Mix‑and‑match: leafy greens + legumes + lean protein + enriched grains covers B‑vitamin bases without megadoses. [4][5][3]
What supplements can (and cannot) do
• Supplements reliably lower the homocysteine number but—outside special situations—haven’t convincingly reduced heart attack or all‑cause cardiovascular events in fortified populations. [9][10][11]
• Stroke reduction is more likely in low‑folate regions. Use supplements to correct deficiencies or when your clinician advises, not as a stand‑alone “heart fix.” [11][12]
When to talk with your clinician (and what to ask)
• Vegan/vegetarian, age ≥60, GI conditions, or on metformin/PPIs? Discuss B12 status. [3]
• Planning pregnancy? Ensure 400 mcg/day folic acid regardless of MTHFR status. [18]
• Family/personal history of premature vascular disease or features of homocystinuria? Ask whether targeted evaluation is warranted. [7]
Key takeaways
• Elevated homocysteine is a risk marker; lowering it with B‑vitamins doesn’t reliably prevent heart attacks in fortified countries like the U.S. [9][10][11]
• Routine MTHFR testing for cardiovascular risk isn’t recommended. [16][17][18]
• Food‑first B‑vitamin strategy (folate, B12, B6) supports healthy metabolism and is easy to do with Illinois grocery options. [4][5][3]
📚 References
- Illinois Department of Public Health. Heart Disease & Stroke – Illinois Statistics (2021). #1
- Centers for Disease Control and Prevention (CDC). Heart Disease Mortality — State Data (2025). #2
- NIH Office of Dietary Supplements. Vitamin B12 – Health Professional Fact Sheet. #3
- NIH Office of Dietary Supplements. Folate – Health Professional Fact Sheet. #4
- NIH Office of Dietary Supplements. Vitamin B6 – Health Professional Fact Sheet. #5
- Linus Pauling Institute (Oregon State University). Vitamin B12: Micronutrient Information Center. #6
- StatPearls. Hyperhomocysteinemia. National Center for Biotechnology Information (NCBI). #7
- Karger A.B., et al. “Association Between Elevated Total Homocysteine and Cardiovascular Outcomes.” Journal of the American Heart Association (JAHA), 2025. #8
- Lonn E., et al. “Homocysteine Lowering with Folic Acid and B Vitamins in Vascular Disease (HOPE-2).” New England Journal of Medicine, 2006. #9
- Bønaa K.H., et al. “Homocysteine Lowering and Cardiovascular Events After Myocardial Infarction.” New England Journal of Medicine, 2006. #10
- NIH ODS. Folate Fact Sheet – Cardiovascular Disease & Stroke Section. #11
- ACC/AHA. 2019 Guideline on the Primary Prevention of Cardiovascular Disease. Journal of the American College of Cardiology. #12
- Markus H.S., et al. “Common MTHFR Mutation and Enzyme Activity.” Stroke, 1997. #13
- Weisberg I., et al. “A1298C Polymorphism Reduces MTHFR Activity.” American Journal of Human Genetics, 1998. #14
- CDC. Impact of U.S. Folic Acid Fortification and Neural Tube Defect Reduction. MMWR, 2010. #15
- American College of Medical Genetics and Genomics (ACMG). Practice Guideline: Lack of Evidence for MTHFR Polymorphism Testing. Genetics in Medicine, 2013. #16
- Deloughery T.G. “MTHFR Polymorphisms Should Not Be Part of Inherited Thrombophilia Testing.” Blood Advances / PMC Review, 2022. #17
- Centers for Disease Control and Prevention (CDC). Folic Acid Clinical Overview – No Recommendation for Routine MTHFR Genotyping. #18
- Centers for Disease Control and Prevention (CDC). Health Equity and Folic Acid Fortification in Corn Masa Flour. Updated 2025. #19